
Cervical cancer - the most important information
Almost 85 percent cases of this disease are recorded in the countries of the Global South. Poland is a country with an average incidence of cervical cancer, but we should not underestimate cervical cancer - in 2019 it was the cause of death of 1,569 Polish women. Most cases occur between the ages of 45 and 55, but younger women are also affected.
In 2019, 2,407 Polish women were diagnosed with cervical cancer, and 1,569 women died from it. The incidence of cervical cancer in Poland is about 15% higher than in Poland. higher than the average for European Union countries.
The mortality rate is even worse. In Poland, it is 70 percent higher. higher than the EU average. These differences result primarily from the universality of women reporting for screening tests - in Poland, about 27 percent of women do cytology. women, while, for example, in Great Britain it is 78 percent, and in Sweden even 90 percent. women.
This cancer develops so slowly that regular (every 1-3 years) cytology allows to detect it at an early stage, when it is almost 100 percent. curable.
Squamous cell cervical cancer
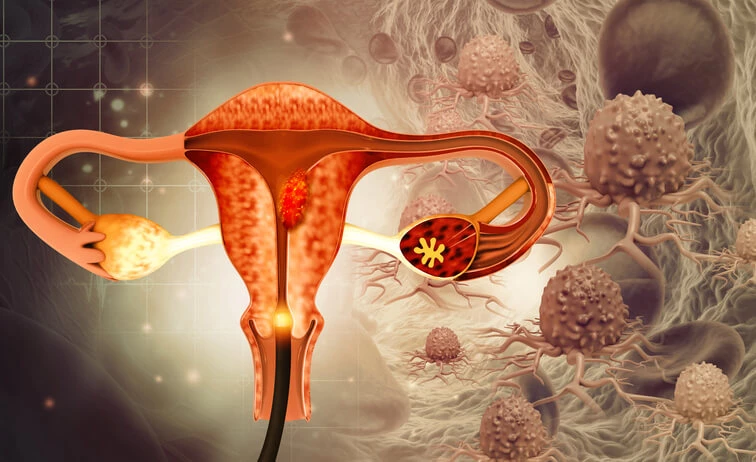
Cervical cancer most often develops on the outer part of the cervix, located in the vagina and called the vaginal disc. This is where the boundary between the two types of epithelium runs:
- glandular epithelium lining the uterine cavity and cervical canal,
- squamous epithelium – covering the vaginal part of the cervix and the vagina.
It is this place, called the transformation zone, that is where cervical cancer develops. It can form from both epithelial cells, but squamous cell carcinoma is much more common.
Causes of cervical cancer
The main cause of this cancer is persistent HPV infection - the genetic material of this virus has been observed in nearly 100 percent. cervical neoplastic tumors examined.
The HPV virus, also called the human papilloma virus, is transmitted sexually, but also through skin-to-skin contact of the genital area. It has also been shown that it can be present on sex toys, which is why it is so important to wash them properly after use. The use of condoms reduces the risk of infection with this virus, but does not guarantee 100% protection. protection.
It is estimated that up to 80 percent of sexually active women are exposed to at least one type of the virus during their lifetime. Despite the prevalence of HPV infection, cancer is a very rare consequence of it. In most cases, infections are transient, but do not confer immunity to subsequent infections, even with the same type of HPV. There are many types of this virus, but only some of them are responsible for the high risk of developing cancer. Other types cause, for example, genital warts, i.e. viral warts of the genital area.
Persistent HPV infection is associated with the development of not only cervical cancer, but also cancer of the vulva, vagina, anus, and in men - cancer of the anus and penis.
The development of cervical cancer is mainly caused by situations that increase the risk of HPV infection (such as a large number of sexual partners or long-term use of contraception, which often goes hand in hand with not using condoms) and those that increase the risk of infection turning into a persistent infection ( such as immunosuppressive treatment). There is no familial predisposition for this cancer.
Risk factors for developing cervical cancer include:
- weakened immunity (e.g. immunosuppressive treatment or HIV infection),
- some genital infections (chlamydiosis, gonorrhea, genital herpes),
- multiple pregnancies and deliveries (more than 5),
- diet low in vitamin C,
- previously found abnormality in the cytological examination,
- smoking tobacco,
- long-term use of hormonal contraception,
- early start of sex life,
- a large number of sexual partners,
- multiple sex partners or HPV-infected themselves.
Symptoms of cervical cancer
The early form of cervical cancer does not cause any symptoms, and it can be detected only thanks to regularly performed, every 1-3 years, cytological tests.
More advanced cervical cancer may present with:
- spotting between periods or after menopause - spontaneous or after intercourse,
- profuse discharge with a characteristic smell,
- pain in the lower abdomen or in the lumbar region.
Other symptoms of advanced cervical cancer:
- frequent urination,
- urinary urgency
- retention of urine in the bladder,
- constipation,
- urge to stool or difficulty passing it.
These symptoms indicate the presence of metastases in the bladder or rectum.
The appearance of bleeding between periods is always a serious signal that may indicate irregularities and, like other disturbing symptoms, requires quick medical control.
Treatment of cervical cancer
The choice of treatment method for cervical cancer depends on the stage of the disease, as well as on the woman's procreation plans. In the treatment of this cancer is used:
- surgical treatment (removal of the cervix or removal of the entire uterus),
- radiotherapy (brachytherapy, i.e. irradiating the tumor from the inside and teletherapy, i.e. irradiating it from the outside),
- chemotherapy,
- radiochemotherapy, ie a combination of radiotherapy and chemotherapy, which aims to increase the effectiveness of both methods.
In the process of treating some patients, it may be necessary to use several methods.
If the cancer is diagnosed at an early stage and a woman wishes to be able to become pregnant in the future, doctors may decide to remove the cervix alone (surgical conization). For patients who do not wish to retain fertility, treatment is based on hysterectomy. In more serious cases, the uterus is removed along with the appendages and lymph nodes.
Operations can be performed in various ways - by opening the abdominal cavity (laparotomy), laparoscopically or with the help of the daVinci robot.
In cases of advanced cervical cancer, radiochemotherapy is the main method of treatment, however, in some patients, surgical treatment is also possible.
Radiotherapy is sometimes used as a complementary treatment after surgery in patients with risk factors for recurrence.
Chemotherapy is mainly used as a palliative treatment, for distant metastases or in case of disease recurrence.
Cervical cancer research
Cytology
Squamous cell carcinoma, which is the most common, is easily detected during cytology. It is a non-invasive and painless test performed by a gynecologist or midwife. It involves collecting cells from the surface of the cervix with a special brush.
For 48 hours before cytology, a woman should refrain from sexual intercourse, vaginal irrigation, and the use of medications or vaginal ointments.
Cytology performed regularly, depending on individual indications, but not less frequently than every 1-3 years, is the best method of detecting cervical cancer at an early stage and allows for prompt implementation of appropriate treatment. Cytology should be performed by all women up to the age of 70 and teenagers who have started intercourse (the first cytology should be performed no later than after the age of 25).
Liquid cytology
Unfortunately, in the case of adenocarcinoma, classical cytology is not very effective. This is because the cancer often grows deep inside the cervical canal, where it is more difficult to obtain the material needed for examination. Other causes of many false-negative results include incorrect smear collection, resulting in a lack of reliable material, and difficulties in interpreting the appearance of these cell types.
A much better method for diagnosing this cancer is liquid cytology based on thin, single-layer cell smears. Unfortunately, this method is not widely available as a screening test, which makes it costly to perform.
Cytology results
Cells collected during cytology are examined in the laboratory and described according to a special scale, thanks to which all cytology results can be compared, regardless of where they were collected. In the past, the so-called Papanicolau scale, which assigned cells to one of five groups.
The more detailed Bethesda system is now used. It gives information not only about the appearance and structure of the cells, but also about the quality of the collected material (whether it is suitable for a reliable assessment) and possible infections.
The table below describes the individual cytology results, both in the Bethesda system and the Papanicolau scale.
| Papanicolau | Bethesda | Other | ||
| Correct image | I | NILM | ||
| Mild changes | II | Reactive changes | ||
| Abnormal epithelial cells | ASCUS/ASG | |||
| III | LSIL/HPV | Low grade dysplasia | CIN I | |
| HSIL | Moderate dysplasia | CIN II | ||
| IV | High-grade dysplasia = pre-invasive cancer | CIN III | ||
| V | Invasive cancer |
- NILM - no suspicion of intraepithelial neoplasia or cancer;
- reactive changes - changes caused by, for example, radiotherapy, chemotherapy or inflammation;
- ASCUS/ASG – atypical squamous cells of undetermined significance or where HSIL cannot be ruled out;
- LSIL/HPV – low-grade endothelial changes in the squamous epithelium;
- HSIL – high-grade endothelial changes in the squamous epithelium.
HPV DNA testing
Pap smear can be supplemented with HPV DNA testing. It allows to diagnose infection with this virus and determine its type (high or low oncogenic). It is recommended for women over 30 because younger women have a better chance of fighting the infection on their own. This test can be combined with liquid cytology and both tests can be taken at the same time (this is the so-called LBC cytology with HPV DNA testing).
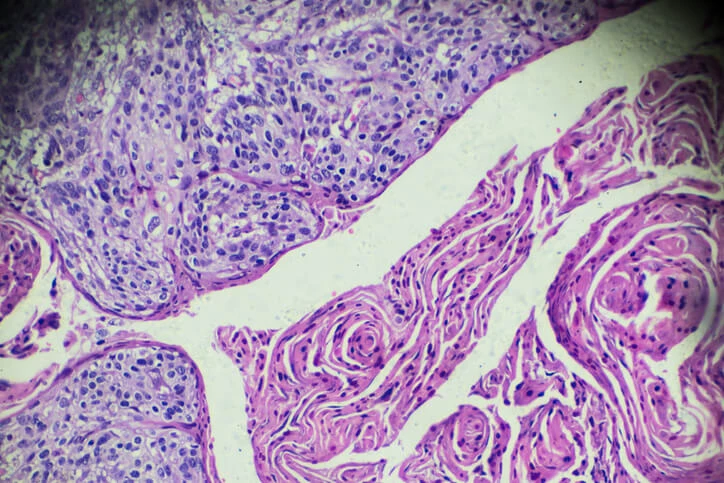
Cervical epithelial cells. What affects the risk of developing cervical cancer? And when is the treatment applied?

Colposcopy
When the cytology result is unclear or abnormal, a colposcopy is performed. It is a test that allows you to view the surface of the vaginal part of the cervix at a magnification of 6 to 40 times and to collect material for histopathological examination from the most "suspicious" place.
In addition, they can be extended with a test with acetic acid, Lugol's solution or toluidine blue, which allows to distinguish between squamous and glandular epithelial cells and to clarify the diagnosis.
The final diagnosis is made on the basis of histopathological examination of the cervical specimen taken during colposcopy. Its result additionally provides information about the advancement of neoplastic changes.
The stage of advancement is determined according to the FIGO scale, i.e. the International Federation of Gynecology and Obstetrics.
Degree | Characteristic |
0 |
|
I |
|
II |
|
III |
|
IV |
|
Based on: Gynecology. Manual for midwives, nurses and physiotherapists, edited by Tomasz Opala.
Tumor markers in cervical cancer
In the case of cervical cancer, tumor markers (such as SCCAg or CA 125 antigen) are selected depending on the type of cancer and are mainly used in prognosis and monitoring the course of the disease, not in its diagnosis.
Expression of p16 and Ki-67 proteins
This test detects cervical cells that have become more severely affected by HPV infection. It plays a big role in ambiguous cytology results, such as ASCUS or LSIL.
Check out Medicover's cancer diagnosis offer >>
Prognosis and complications of cervical cancer
Cancer detected at an early stage is nearly 100% curable. curable. In stage III, the 5-year survival rate is only 30-40%, and in stage IV it is even lower.
A complication of cervical cancer is the appearance of metastases, most often in the liver, bones, lungs and intestines. Metastases indicate a high advancement of the disease and their appearance reduces the chance of full recovery.
Cervical cancer prevention - how to prevent?
The best method of cervical cancer prevention is regular cytology every 1-3 years.
There is a special cervical cancer prevention program in Poland. As part of it, every woman between 25 and 59 years of age has the right to free cytology once every 3 years. This examination is paid for by the Ministry of Health.
A revolution in the prevention of cervical cancer is the introduction of the HPV vaccine, which reduces the risk of infection with some types of the virus by over 75%. Not only girls but also boys should be vaccinated because they also need protection against HPV.
The Polish Protective Vaccination Program recommends vaccinating people from the age of 9 against HPV, but even women up to the age of 45 can benefit from vaccination, so it is worth discussing this topic during the next visit to the gynecologist or midwife.
Check out Medicover's cancer prevention offer >>
Remember
- Regularly, every 1-3 years, perform cytology.
- If you do not have a permanent partner or you are not sure if your partner is faithful to you, always use condoms during sexual intercourse, which will reduce the risk of HPV infection.
- If you are before sexual initiation or you are under 45 years old, get vaccinated against HPV after consulting a gynecologist.
Medicover offer
|
The presented medical information should not be treated as guidelines for medical conduct in relation to each patient. The medical procedure, including the scope and frequency of diagnostic tests and/or therapeutic procedures, is decided by the doctor individually, in accordance with medical indications, which he determines after getting acquainted with the patient's condition. The doctor makes the decision in consultation with the patient. If the patient wants to perform tests not covered by medical indications, the patient has the option of paying for them. |

Prezentowanych informacji o charakterze medycznym nie należy traktować jako wytycznych postępowania medycznego w stosunku do każdego pacjenta. O postępowaniu medycznym, w tym o zakresie i częstotliwości badań diagnostycznych i/lub procedur terapeutycznych decyduje lekarz indywidualnie, zgodnie ze wskazaniami medycznymi, które ustala po zapoznaniu się ze stanem pacjenta. Lekarz podejmuje decyzję w porozumieniu z pacjentem. W przypadku chęci realizacji badań nieobjętych wskazaniami lekarskimi, pacjent ma możliwość ich odpłatnego wykonania. Należy potwierdzić przy zakupie badania szczegóły do jego przygotowania. |